- Health Distilled by Liverpool Lane
- Posts
- University innovation ranked, hospital employment and innovation, optionality and more.
University innovation ranked, hospital employment and innovation, optionality and more.
Healthcare through a Kentucky lens. Yeah, it's niche. But neat!
Andrew Steen
May 19, 2026

🧑🎓
Cure Innovation Index
“The Cure Innovation Index is the first evidence-based ranking of U.S. research institutions — built to identify, measure, and evaluate what it takes to turn scientific discovery into real healthcare solutions.” Worth a read, including this subsection.
Overall, how did the Commonwealth fare?

The AI-Powered Payer
From Innovaccer’s The AI-Powered Payer: Leaders’ Perspectives for 2026:

“The findings mark a significant shift from prior industry surveys, which found a majority of payers building AI capabilities internally.”
Hospital Employment
This is hopefully the start of a connected thought thread.
“Hospitals are the sixth largest employer in the country, and among the top five largest employers in 22 states, when comparing industry subsectors,” shares KFF.

Hospitals are among the top five largest employers in Kentucky. 95,942 people. I am willing to bet those people have innovative ideas in them. Maybe even a startup or two.
Hospitals have a big economic impact in Kentucky.

However…

Again, lean into hospital employees.
How about a hackathon?
Our findings suggest that hackathons support corporate innovation by enabling rapid experimentation, attracting entrepreneurial talent, and cultivating internal knowledge-sharing communities.
Problems operators are actually trying to solve
Ballad Health again.
“In the coming weeks and months, we'll be posting specific problems to solve and challenges that our leadership has identified.” So good.

Louisville. No reason you couldn’t do something like this.
An AI-powered primary care doctor
I thought this was interesting. Big pre-seed round.
-1200x630.png)
What does a local internal medicine physician think about it?
So first of all I do like AI in medicine, as it can collate significant amounts of information and could help with developing retrospective studies to help with answering some anecdotal observations in practice. What Clara is wanting to do is a little more dangerous as EHRs for hospitals/office settings are notorious for having their problem list, medication list, and preventative therapies not updated. This could lead to notifications about med refills for therapeutics patients are no longer taking or even worse, could be contraindicated now that the patient has started some other non-reported med. The EHR is only as good as the people reviewing the data and keeping it updated, which, unfortunately happens very sporadically. If--and it is a very big if--all EHRs communicated seamlessly with pharmacy databases and all old meds and diagnoses purged as soon as they were obsolete, then maybe it would be helpful to a primary care doctor. But to take the place of a primary provider, I think we are a long way away from this.
Swamp Night
From our friends at KYX. Navigating the Louisville entrepreneurial ecosystem.

Related, this by Paul O'Brien. Spot on for Louisville. Please read it.
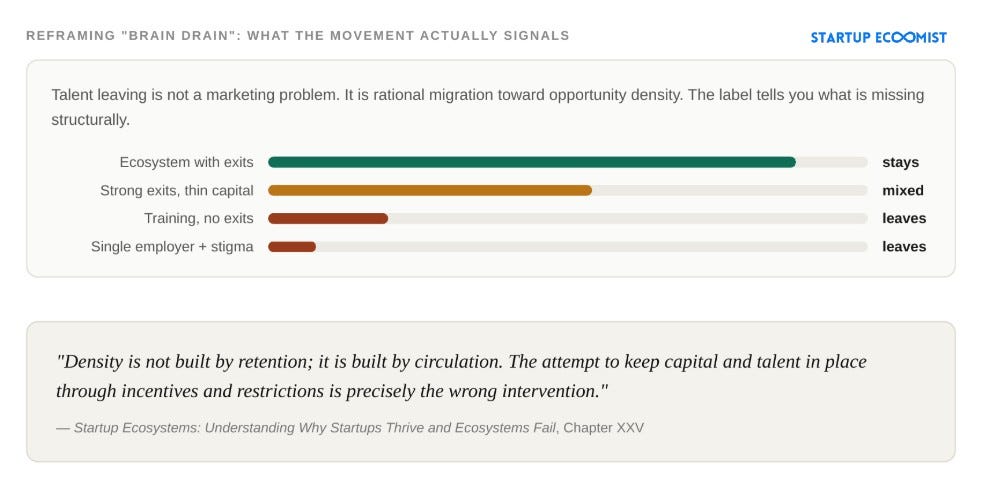
Connecting the people building the future of healthcare in Louisville.
Join in.